Camouflaging Skeletal Discrepancy with Dental Movements
By: Dr. Bryan Lockhart, DDS
Orthodontic treatment for adults presents unique challenges and considerations due to factors like missing teeth, extensive restorations, periodontal concerns, and patient compliance. Unlike growing patients, adults cannot rely on growth to aid in malocclusion correction. Additionally, adult patients often prioritize shorter treatment times and minimal social impact. This article explores a case study of a 22-year-old adult female with a Class III malocclusion and outlines the treatment approach, challenges, alternatives, and outcomes.

Case Presentation and Diagnosis
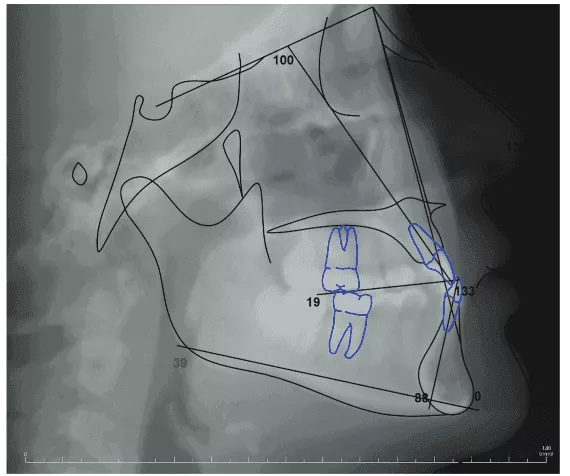
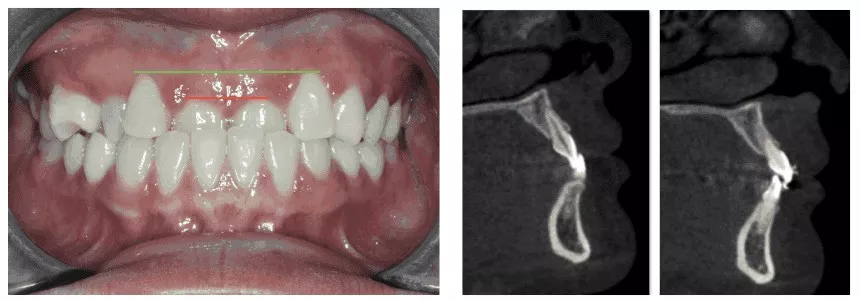
The patient, a 22-year-old adult female, expressed dissatisfaction with her two front teeth, which were positioned behind her lower front teeth. She exhibited a Class III concave profile with a mildly retrognathic maxilla. Dentally, she had a Class III molar relationship, an anterior crossbite involving maxillary central incisors and a maxillary right canine, retroclined maxillary and mandibular incisors, a 3mm mandibular curve of Spee, supra-erupted maxillary central incisors, and a maxillary right first premolar rotated nearly 90 degrees. Additionally, uneven gingival zeniths were observed, mainly due to the supra-erupted central incisors.
This case posed a unique challenge because the patient's mild skeletal Class III malocclusion did not warrant orthognathic surgery. Alternative solutions were sought to address the skeletal issue through dental movements only, which is known as camouflage treatment. Managing the patient's expectations was crucial, as she desired a "perfect" smile, limited by factors like periodontal support, tooth shape, size, and color. Explaining the non-surgical approach was essential for achieving a result that satisfied the patient.
Treatment Objectives
Correct the anterior crossbite.
Resolve maxillary and mandibular crowding.
Achieve a Class I molar relationship.
Improve maxillary incisor torque.
Treatment Alternatives
The primary alternative was surgical intervention, involving maxillary premolar extractions and LeFort I maxillary advancement. However, the patient preferred a non-surgical approach.
Treatment Plan
The chosen treatment plan aimed to align the maxillary and mandibular teeth, correct the anterior crossbite through maxillary central incisor proclination and intrusion, and level the maxillary anterior gingiva. The excessive mandibular curve of Spee would be corrected by leveling the lower arch and using Class III elastics for sagittal correction.
Treatment Plan Sequencing
The patient was offered various treatment options, including metal braces, clear/ceramic braces, or clear aligners. She opted for ceramic braces due to concerns about compliance with clear aligners while still seeking a more esthetic alternative to metal braces.
The patient was bonded with Symetri™ Clear brackets (Ormco) with an MBT prescription and a 0.022 slot. Bite turbos were placed on the lower central incisors, and light wires (0.014 nitinol) were used to align the maxillary right first premolar gently. Lingual buttons were placed on the lingual surface of the first and second maxillary right premolars, and power chains assisted in derotating the maxillary first premolar.
Archwires were advanced to 0.018 NiTi, and Class III elastics were introduced. Archwire sizes were increased to .021″ x .025″ NiTi to achieve greater buccal crown torque on the maxillary incisors. The elastics' sizes were increased to 3/16 heavy on the right side only, achieving proper angulation while preserving bone facial to the central incisor roots.
Outcome of Treatment
The treatment resulted in a successful outcome, achieving Class I molars, correcting the anterior crossbite, and obtaining positive overjet. The patient completed treatment in 19 months, which aligned with her desire for shorter treatment duration. While some aspects could have been improved, such as settling the occlusion on the right side and coordinating midlines better, the patient was content with the progress and outcome.
In summary, this case demonstrates the challenges and complexities of adult orthodontic treatment, particularly when camouflaging a mild skeletal Class III malocclusion. Effective communication, proper treatment planning, and patient compliance are essential in achieving successful outcomes. Despite some areas for improvement, the patient's satisfaction and shorter treatment time highlight the positive aspects of the treatment approach.

Author: Dr. Bryan Lockhart, DDS
Originally from Decatur, Georgia, Bryan Lockhart, DDS, attended the University of North Carolina at Chapel Hill for dental school. He attended a 1-year General Practice Residency at Montefiore Medical Center in New York before obtaining his Certificate in Orthodontics from Jacksonville University in Jacksonville, Florida. Dr. Lockhart furthered his learning by attending Jacobi Medical Center for an Orthodontic/Orthognathic Surgical Fellowship. Dr. Lockhart is well versed in fixed appliances as well as clear aligners and has developed his own clear aligner brand, Dualine. Dr. Lockhart is a member of SAO, AAO, and is board-certified with the American Board of Orthodontists (ABO). He has two orthodontic offices in Charlotte, North Carolina, where he practices with his wife, Dr. Lauren Lockhart.

