Case Study: Earned Placement- Clinical Efficiency With ‘True Straight Wire’
By Dr. Frank Bogdan
Ever since Larry Andrews published “The Six Keys to Normal Occlusion” in the AJO-DO in 19721 (the second year of my residency at the University of Medicine and Dentistry of New Jersey, now Rutgers), it was apparent to me that straight wire was the way to go in clinical practice.
Upon graduation, I went with a company that made Andrews’ bracket prescription built into the base of an edgewise bracket with a 0.022-by-0.028-inch slot. The tip and torque required for each tooth was based on untreated cases from which Andrews developed his “six keys of occlusion.”
The Andrews appliance proved to be a big advantage over the plain vanilla edgewise brackets I used in residency. However, I soon discovered I was never going to finish a case in a straight wire, because individual cases would still require first-, second- and third-order bends to finish. The preadjusted appliance did give the profession a head start to finishing, but still had shortcomings.
Over the next 20 years, I played around with various prescriptions in an attempt to do less wire bending and increase efficiency with some success. I settled with a Roth prescription (modified). The maxillary canines (–7) did not create the aesthetic, broad smile I was looking for in my cases. The canines always required positive torque in the finishing stage and therefore required modifying. In addition, I used a great deal of functional appliances (Frankel, Activator, Bionators, Twin Block and Herbst) to achieve better results with fewer extractions.
Light Force Meets Low Friction
In the 1990s, my orthodontic career took a major turn with Ormco buying the company I mentioned above. In 1997, I was looking to change my appliance from a single-wing edgewise bracket to an edgewise twin bracket. As fate would have it, I took a course in New Orleans with Dr. Dwight Damon, who had a new passive self-ligating (PSL) bracket system. Two hours into the lecture, I knew for the first time in my career that I was going to make a total system change to passive self-ligation.
I was impressed with the tooth movement I was seeing in Damon’s cases when light force (delivered by superelastic wires) and low friction (PSL brackets) were combined. A few years later, as I utilized the system, I realized that muscles were affecting my cases like “functional” appliances because of lower friction: The tongue muscle was able to aid expansion of the arches by uprighting the buccal segments previously overpowered by a strong buccinator and orbicularis muscles. Our office visits were pushed out to eight to 10 weeks, and cases were treating out faster, with fewer office visits and fewer extractions, because of what I described at the time as “arch width development.” It was similar to the tooth movement I’d previously seen in Frankel cases2 and described by Melvin Moss as “teeth uprighting over their apices in a functional matrix.” 3 Today, Dr. Tom Barron and I describe the movement as alveolar bone modeling (increase in bone volume), detailed in an article we wrote for Clinical Impressions in the summer of 2017: “These processes are well-accepted phenomena in the field of physiology.”4
Unique in this passive self-ligation straight-wire system was the introduction of selective torques. They included standard (similar to Andrews’ script), high-torque and low-torque brackets that were color-coded blue, red and green respectively, so cases could be “scripted.” The concept allowed increased efficiency by utilizing torques to offset the side effects of treatment mechanics. For example, in a Class II case, high-torque brackets on upper anterior teeth and low torque on the lower anterior teeth help keep the teeth upright, because the mechanics will retrocline upper anteriors and procline the lower anteriors. The reverse script would be utilized in Class III cases to offset the opposite mechanical side effects.
One problem with all straight-wire brackets is the play in the slot. A 0.019-by-0.025-inch wire in a 0.022-by-0.028-inch slot has nearly 12 degrees of play in either direction in a standard bracket. The play affects tooth control in all three planes of space, with the most noticeable in my opinion being torque and rotation control. Utilizing pretorqued brackets high or low reduces play but does not allow center slot alignment because the torque is in the base; therefore, finishing in a straight wire is virtually impossible. Wire bending and/or bracket repositioning is necessary and challenging without center slot alignment, hence all the complaints of cases being difficult to finish in the use of a passive self-ligation system. All of the above will reduce efficiency in treatment.
Synopsis
The problem: Play in the slot must be reduced without dramatically increasing friction. Increasing wire size (to fill the slot and expression) does increase friction (static and binding) as well as patient discomfort with insertion (big wires hurt) and finishing bends.
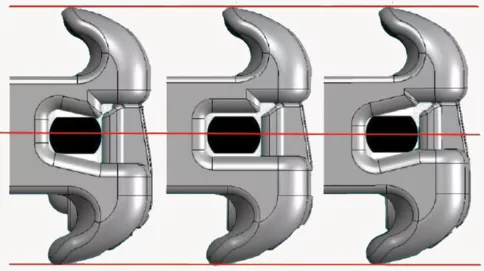
The solution: The Ultima bracket and wire assembly. Damon Ultima is the latest-generation Damon system, made of an assembly consisting of the Ultima bracket and Ultima wire. The bracket is a passive self-ligating bracket with a parallelogram-shaped slot, available across retrocline and procline prescriptions. The wire is a proprietary round-sided rectangular archwire with a depth of 0.0275 inch, compared with traditional 0.025-inch depth archwires. When this archwire is engaged in the paralellogram bracket slot, there are four contact points between wire and slot—two vertical, two horizontal—and these contact points allow the clinician to deliver full control over rotation, torque and angulation. This full expression assembly allows me to treat cases more predictably, with fewer visits and manual adjustments, while maintaining clinical excellence in my finishes. (See Figs. 1–3, courtesy of Ormco.)
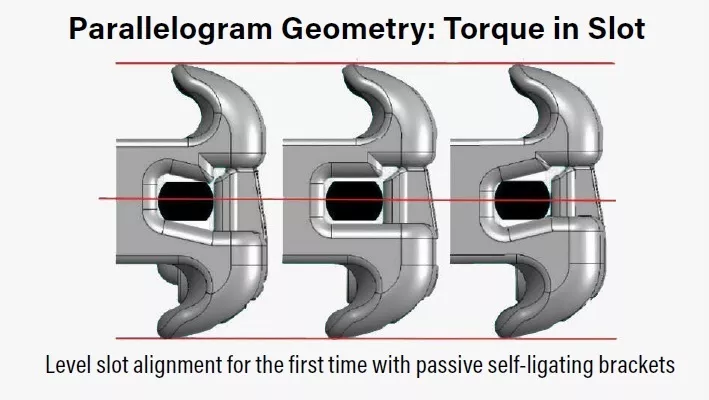
FIG. 1
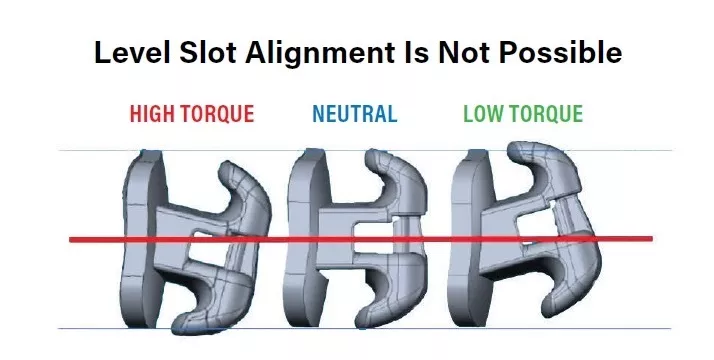
FIG. 2
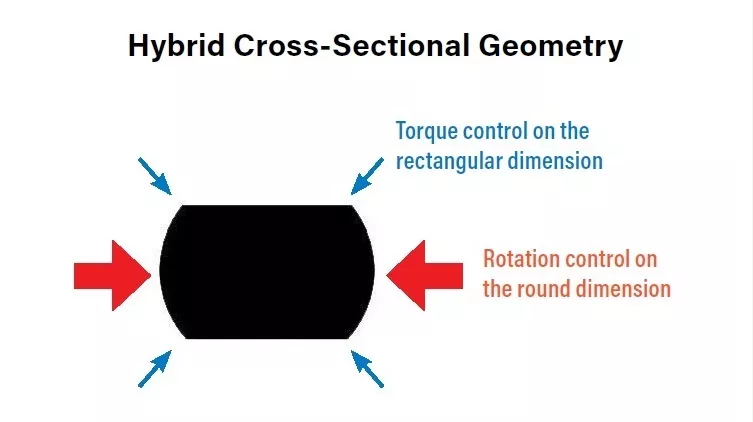
FIG. 3
Case 1: Class II End-On
Damon Ultima Brackets
This patient came in with a Class II end-on malocclusion. We began using the Ultima bracket in spring 2021 and started the patient with maxillary anterior rotations. The rotation control with the Ultima bracket system was impressive (Figs. 4 and 5). Rotation correction is generally finalized after 10 weeks in the 0.014-by- 0.02175- inch nickel-titanium combination wire, as seen in the side-by-side maxillary occlusal photos in Fig. 6. The patient was reasonably compliant with Class II elastics, and the case finished (Fig. 7) in 16 months and 10 office visits, including the strap-up, reposition and debonding visits. Only one detail bend (Fig. 8) was required between the maxillary centrals to finish. Using Ultima has increased our office efficiency.

Fig. 4

Fig. 5

Fig. 6

Fig. 7

Fig. 8
The result: A potentially pure straight-wire (preadjusted) appliance is born. If the finishing wire is straight and if any teeth are not aligned, the bracket position is off and easily identified for reposition. Additional torque expression (if needed) can be delivered with “overdrive wires” (0.019, 0.020 or 0.021 by 0.0275 inch).
The bottom line: I am now utilizing a straight-wire appliance that has full expression, delivers light force and has three-dimensional control designed to treat in less time (according to data on file at Ormco). It took a lot of years to get here but, in my opinion, we finally have a true straight-wire system.
Case 2: Pseudo Class III
A 40-year-old patient (Figs. 9 and 10) presented with a Class III malocclusion, with a maxillary anterior crossbite, right-side posterior crossbite of the second premolar through the second molar and on the left side, a posterior crossbite and open-bite tendency of the molars. In addition, the arch form was poor, with a functional shift to the left side.
This case dramatically illustrates the clinical efficiency of the new Ultima system, the alveolar bone modeling of the Damon system in nongrowing adult dentitions and significant transverse development of the arches.
Dr. Hisham Badawi said it best: “Dwight [Damon], you have succeeded in filling the slot without filling the slot.” In short, the combination wire in the unique (parallelogram) slot shape of the Ultima bracket allows us much better control without losing the advantage of the muscles helping us treat the malocclusion with PSL, in growing and nongrowing patients alike. The before and after photos (Fig. 11) speak for themselves.
The case was completed in 14 months without surgery and with only nine office visits. The patient was compliant with light crossbite and Class III elastics and has a life-changing result. There were a few finishing bends needed in the Damon Clear brackets on the maxillary anteriors.

Fig. 9

Fig. 10

Fig. 11
References
1. Andrews, L. “The Six Keys to Normal Occlusion.” AJO-DO, Sept. 1972, pp. 296–309.
2. Frankel, R. “The Practical Meaning of the Functional Matrix in Orthodontics.” Transactions of the European Orthodontic Society 45 (1969): pp. 207–219.
3. Moss, M. “The Functional Matrix” (chapter), Vistas in Orthodontics. Lea and Fibiger, 1962.
4. Barron, T., and Bogdan, F. “A Practical Treatment Objective: Alveolar Bone Modeling With a Fixed, Continuous- Arch Appliance.” Clinical Impressions, 20:1, Summer 2017.
Dr. Frank Bogdan is a paid consultant for Ormco. After treating patients for many years at his practice in New Jersey, Bogdan focused on teaching the next generation of orthodontists, which allowed him to travel and make friends across the world. He has since retired from orthodontic practice and moved to Florida, where he lives with his wife, Diane.


